What is ERCP





What is ERCP

What is ERCP? What are the causes of the biliary obstruction?
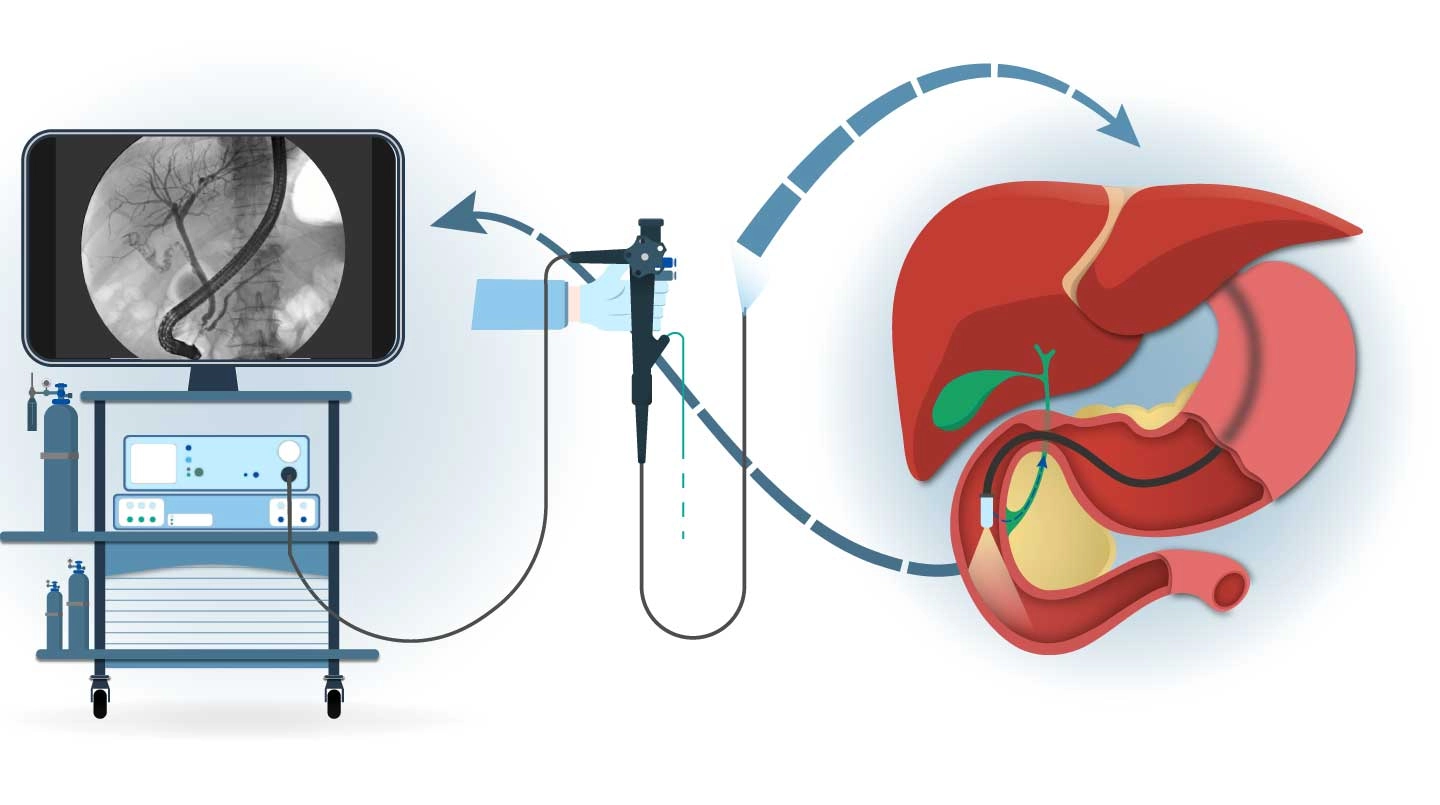
Ercp is a word created from the initials Endoscopic Retrograde Cholangio Pancreotography. By going to the area where the bile ducts flow with the endoscopic method, the image of the bile ducts is obtained by entering out of the bile duct by putting the catheter and giving the liquid contrast material that can be seen in the x-ray. Thus, it is understood whether there are stones in the bile ducts or if there is a pressure from any tumour.
In previous years, ERCP was carried out only for the purpose of diagnosing pathologies in the bile ducts but has now taken MRCP or endoscopic ultrasound examinations for this. ERCP is now only available for the purpose of treatment.
The most common use of ERCP is the obstructive jaundice problems made by stones in the bile ducts to the present day. Stones in the bile ducts usually form by falling from the gall bladder to this path. However, especially in people whose gallbladder has been removed before, new stones may form again over time from the bile ducts themselves.
When the stone falls into the bile ducts, the stone leads to the outlet of the bile ducts. And it wants to go from here to the small bowel. Normally, when the bile ducts close the place where the small bowel flows into, it merges with the main canal from within the pancreatic gland. As if the two rivers were flowing out of one mouth, they flow into the small bowel. Therefore, if the stone which falls into the bile tracts comes and cannot pass the exit, it occludes both the bile
Anatomy of the bile duct
The place where the bile ducts open to the small bowel is defined as the papilla. When we look at from the small bowel, the papilla is looked like as the nipple. A very little imperceptible tedge may be seen in the middle of it. There is a space that defined as the ampulla of Vater where the bile duct and the pancreatic duct merge in the inner of this tedge. Stones can occlude both ducts by settling in this area.

The papilla is the point that the bile duct and the pancreatic duct merge and flow into the small bowel.
The common bile duct can also be defined as ductus choledochus. Bilirubin which is a material in the gall cannot pass the little bile ducts in the liver, because when choledochal is occluded by stones, it cannot clear the gall which needs to reach to the small bowel by passing through it. These materials which cannot be thrown to the bile ducts start to pass into the blood. High level of bilirubin in the blood causes yellowing of the whole body, especially skin and eye. It is defined as obstructive jaundice.
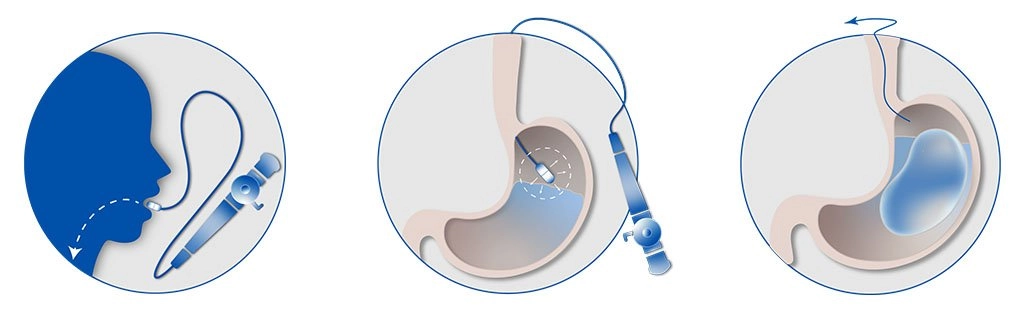
So ERCP not only provides the enlargement by cutting the low end of the bile ducts with a device named as papillotomy especially in the case of occlusion such as stone but also clears these foreign matters from the bile duct with a catheter-like a balloon or a basket. Below, these procedures are showed and explained with the purpose of the information in ERCP that I applied.
WHAT ARE THE PRIMARY CAUSES OF OBSTRUCTIVE JAUNDICE?
- Gallstones in the choledoch
- Tumors of ampulla of vater
- Mass in the head of the pancreas
- Chronic pancreatitis
- of Biliary tract neoplasms
- Binding the common bile duct accidentally during the cholecystotomy
- Mirizzi’s syndrome > occurs as a result of the acute inflammation of gall enters the bile ducts
WHICH TREATMENTS CAN BE APPLIED WITH ERCP?
ERCP can clear the stones which cause the occlusion in the bile duct.
The exit part of the choledochus can be opened by cutting the adenoma of the Vater ampoule, which can cause occlusion.
During the preparation of the operation, temporary catheters of Nazo-biliary drainage may put to reduce the risk of the operation by reducing the levels of high bilirubins at the mass in the head of the pancreas which can cause occlusion.
Permanent stents can put to provide the gall flowing in the advanced bile-pancreatic duct that may be another cause of the occlusion and non-operable.
What is ERCP
What is ERCP? What are the causes of the biliary obstruction?
Ercp is a word created from the initials Endoscopic Retrograde Cholangio Pancreotography. By going to the area where the bile ducts flow with the endoscopic method, the image of the bile ducts is obtained by entering out of the bile duct by putting the catheter and giving the liquid contrast material that can be seen in the x-ray. Thus, it is understood whether there are stones in the bile ducts or if there is a pressure from any tumour.
In previous years, ERCP was carried out only for the purpose of diagnosing pathologies in the bile ducts but has now taken MRCP or endoscopic ultrasound examinations for this. ERCP is now only available for the purpose of treatment.
The most common use of ERCP is the obstructive jaundice problems made by stones in the bile ducts to the present day. Stones in the bile ducts usually form by falling from the gall bladder to this path. However, especially in people whose gallbladder has been removed before, new stones may form again over time from the bile ducts themselves.
When the stone falls into the bile ducts, the stone leads to the outlet of the bile ducts. And it wants to go from here to the small bowel. Normally, when the bile ducts close the place where the small bowel flows into, it merges with the main canal from within the pancreatic gland. As if the two rivers were flowing out of one mouth, they flow into the small bowel. Therefore, if the stone which falls into the bile tracts comes and cannot pass the exit, it occludes both the bile
Anatomy of the bile duct
The place where the bile ducts open to the small bowel is defined as the papilla. When we look at from the small bowel, the papilla is looked like as the nipple. A very little imperceptible tedge may be seen in the middle of it. There is a space that defined as the ampulla of Vater where the bile duct and the pancreatic duct merge in the inner of this tedge. Stones can occlude both ducts by settling in this area.
The papilla is the point that the bile duct and the pancreatic duct merge and flow into the small bowel.
The common bile duct can also be defined as ductus choledochus. Bilirubin which is a material in the gall cannot pass the little bile ducts in the liver, because when choledochal is occluded by stones, it cannot clear the gall which needs to reach to the small bowel by passing through it. These materials which cannot be thrown to the bile ducts start to pass into the blood. High level of bilirubin in the blood causes yellowing of the whole body, especially skin and eye. It is defined as obstructive jaundice.
So ERCP not only provides the enlargement by cutting the low end of the bile ducts with a device named as papillotomy especially in the case of occlusion such as stone but also clears these foreign matters from the bile duct with a catheter-like a balloon or a basket. Below, these procedures are showed and explained with the purpose of the information in ERCP that I applied.
WHAT ARE THE PRIMARY CAUSES OF OBSTRUCTIVE JAUNDICE?
- Gallstones in the choledoch
- Tumors of ampulla of vater
- Mass in the head of the pancreas
- Chronic pancreatitis
- of Biliary tract neoplasms
- Binding the common bile duct accidentally during the cholecystotomy
- Mirizzi’s syndrome > occurs as a result of the acute inflammation of gall enters the bile ducts
WHICH TREATMENTS CAN BE APPLIED WITH ERCP?
ERCP can clear the stones which cause the occlusion in the bile duct.
The exit part of the choledochus can be opened by cutting the adenoma of the Vater ampoule, which can cause occlusion.
During the preparation of the operation, temporary catheters of Nazo-biliary drainage may put to reduce the risk of the operation by reducing the levels of high bilirubins at the mass in the head of the pancreas which can cause occlusion.
Permanent stents can put to provide the gall flowing in the advanced bile-pancreatic duct that may be another cause of the occlusion and non-operable.